Retevmo was evaluated in a phase I/II trial: the largest trial ever reported in patients with RET-driven cancer1-2
796 patients with RET-altered advanced or metastatic solid tumors were included in LIBRETTO-001, an open-label, single-arm, multicenter, phase I/II, multicohort trial.1-5*
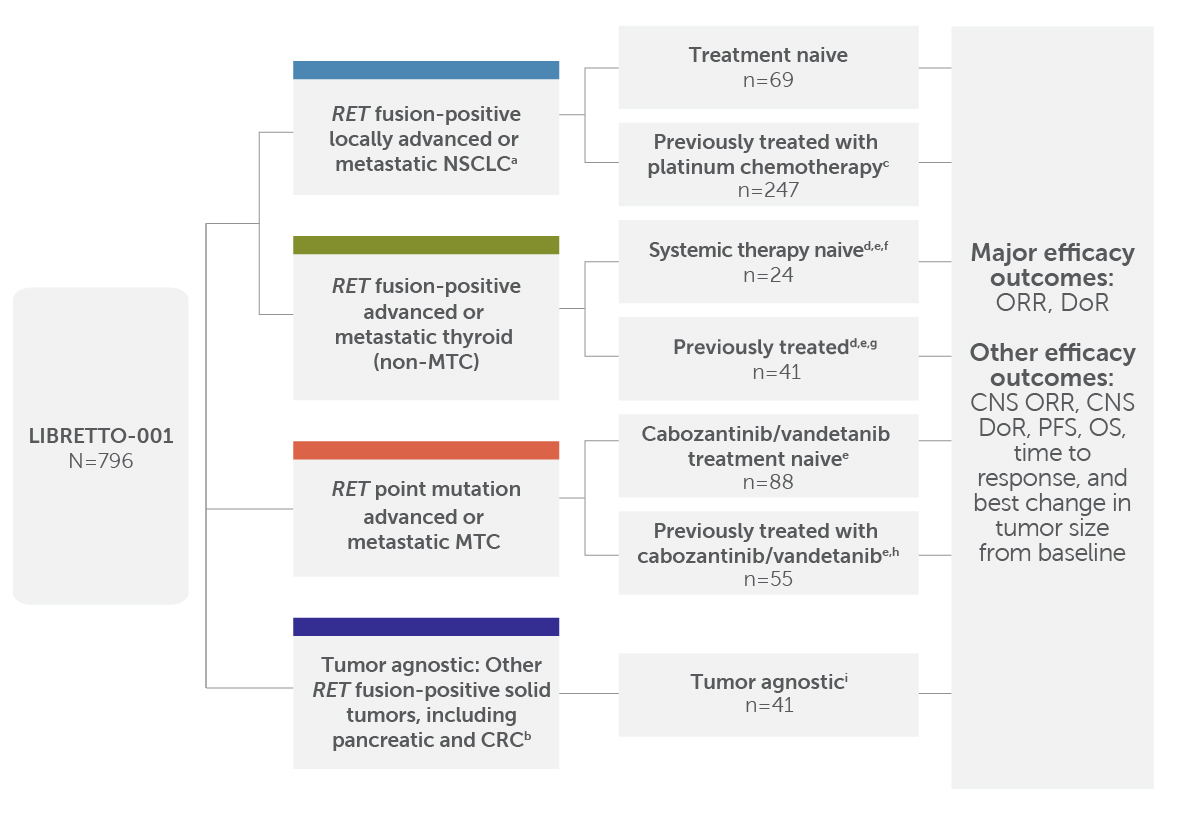
LIBRETTO-001 included 796 patients, and the major efficacy outcomes were ORR and DoR; other efficacy outcomes included CNS ORR, CNS DoR, PFS, OS, time to response, and best change in tumor size from baseline.1,3,5
The study evaluated the following cohorts for efficacy: systemic therapy-naive patients (n=69) and previously treated patients who had progressed on platinum-based chemotherapy (n=247c) with advanced or metastatic RET fusion-positive NSCLC; systemic therapy-naive (n=24d,e,f) and previously treated (n=41d,e,g) patients with advanced or metastatic RET fusion-positive thyroid cancer (non-MTC); patients with advanced or metastatic RET-mutant MTC that were cabozantinib and vandetanib-naive (n=88e) and patients previously treated with cabozantinib and/or vandetanib (n=55e,h); and patients in the tumor agnostic cohort (n=41i). Major efficacy outcomes were ORR and DoR. Other efficacy outcomes included CNS ORR, CNS DoR, PFS, OS, time to response, and best change in tumor size from baseline.
The overall safety analysis included 24 patients with other cancers, including cancers without a RET alteration.4
Phase 1 dose escalation: Retevmo dosed at 20 mg QD–240 mg BID. Intra-patient dose escalation was allowed by protocol.3
Phase 2 dose: Retevmo dosed at 160 mg BID.3
See full Prescribing Information for dosing instructions.
Objective response rate (ORR) was defined as complete response (CR) + partial response (PR) and was assessed by independent review committee (IRC) according to Response Evaluation Criteria in Solid Tumors (RECIST) v1.1.1
The intent-to-treat (ITT) population was analyzed in the LIBRETTO-001 trial because this type of analysis avoids the selective exclusion of patients, which can lead to a biased assessment of an intervention's effectiveness.6-9
aPatients with advanced or metastatic RET fusion-positive NSCLC who had progressed on platinum-based chemotherapy and those without prior systemic therapy were enrolled in separate cohorts.1
bEfficacy was evaluated in 41 patients, including those with the following tumor types: pancreatic adenocarcinoma (n=11); colorectal (n=10); salivary (n=4); unknown primary (n=3); breast (n=2); sarcoma (soft tissue) (n=2); xanthogranuloma (n=2); carcinoid (bronchial) (n=1); carcinoma of the skin (n=1); cholangiocarcinoma (n=1); ovarian (n=1); pulmonary carcinosarcoma (n=1); rectal neuroendocrine (n=1); small intestine (n=1).1
cEfficacy was evaluated in 247 adult patients with advanced or metastatic RET fusion-positive NSCLC who were previously treated with platinum chemotherapy enrolled into a cohort of LIBRETTO-001. All 247 patients received systemic therapy (with a median of 2 prior systemic regimens). 144 of the 247 patients received prior anti-PD-1/PD-L1 therapy, and 85 of the 247 patients received a prior MKI.3
dNon-MTC by histology included papillary (n=54), poorly differentiated (n=6), anaplastic (n=4), and Hurthle cell (n=1).1
eNumber of patients included in the initial efficacy analysis. Efficacy was based on patients who had at least 6 months of follow-up.4
fPatients in this cohort received no prior systemic therapy other than RAI.1
gPatients in this cohort received a prior systemic therapy other than RAI.1
hThe efficacy of Retevmo was evaluated in 55 patients with RET-mutant advanced MTC who were previously treated with cabozantinib or vandetanib enrolled into a cohort of LIBRETTO-001.1
iPatients in this cohort could have received prior systemic therapies with a median of 2 prior systemic therapies (range 0-9).1
*Pooled safety analysis: data as of June 15, 2021
BID=twice daily; CNS=central nervous system; CRC=colorectal cancer; DoR=duration of response; MKI=multikinase inhibitor; MTC=medullary thyroid cancer; NSCLC=non-small cell lung cancer; OS=overall survival; PD-1=programmed cell death 1; PD-L1=programmed death-ligand 1; PFS=progression-free survival; QD=once daily; RET=rearranged during transfection.
Retevmo demonstrated a consistent response in patients with certain RET-driven cancers in the LIBRETTO-001 trial1
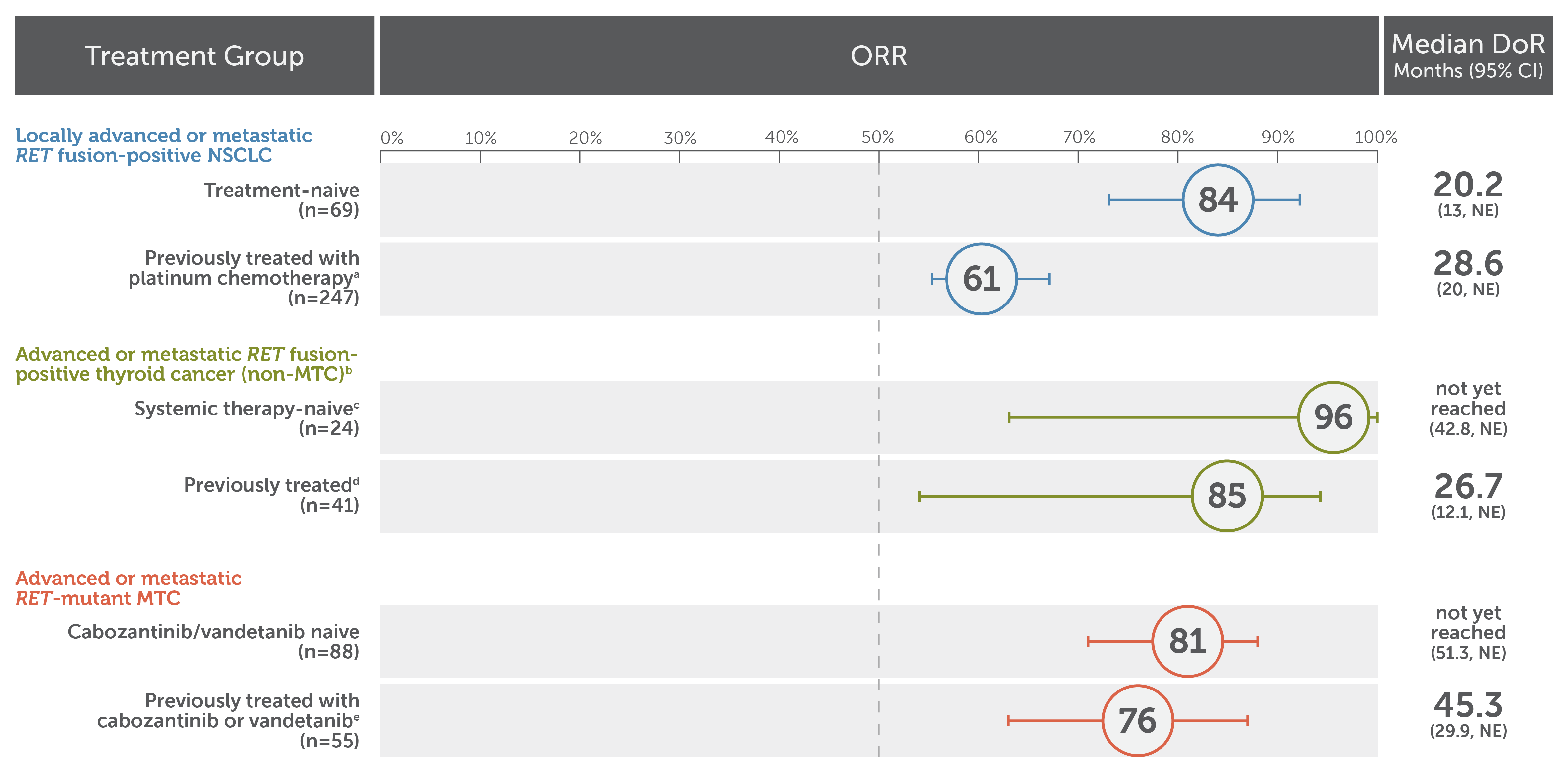
In patients with locally advanced or metastatic RET fusion-positive NSCLC: treatment-naive patients (n=69): 84% ORR (95% CI: 73, 92), median DoR was 20.2 months (95% CI: 13, NE); patients previously treated with platinum chemotherapy (n=247): 61% ORR (95% CI: 55, 67), median DoR was 28.6 months (95% CI: 20, NE).
In patients with advanced or metastatic RET fusion-positive thyroid cancer (non-MTC): systemic therapy-naive patients (n=24): 96% ORR (95% CI: 79, 100), median DoR not yet reached (95% CI: 42.8, NE); previously treated patients (n=41): 85% ORR (95% CI: 71, 94), median DoR was 26.7 months (95% CI: 12.1, NE).
In patients with advanced or metastatic RET mutant-MTC: cabozantinib/vandetanib treatment-naive patients (n=88): 81% ORR (95% CI: 71, 88), median DoR was not yet reached (95% CI: 51.3, NE); patients previously treated with cabozantinib and/or vandetanib (n=55): 76% ORR (95% CI: 63, 87), median DoR was 45.3 months (95% CI: 29.9, NE).
Each paragraph is referenced to: Retevmo (selpercatinib). Prescribing Information. Lilly USA, LLC.
aEfficacy was evaluated in 247 adult patients with locally advanced or metastatic RET fusion-positive NSCLC who were previously treated with platinum chemotherapy enrolled into a cohort of LIBRETTO-001. All 247 patients received systemic therapy (with a median of 2 prior systemic regimens).1
b Primary tumor histologies included papillary thyroid cancer, poorly differentiated thyroid cancer, anaplastic thyroid cancer, and Hurthle cell thyroid cancer.1
c Patients received no prior systemic therapy other than RAI.1
d Patients received a prior systemic therapy other than RAI.1
e The efficacy of Retevmo was evaluated in 55 patients with RET-mutant advanced MTC who were previously treated with cabozantinib or vandetanib enrolled into a cohort of LIBRETTO-001.1
The major efficacy outcome measures in LIBRETTO-001 were ORR and DoR. ORR was defined as CR + PR and was assessed by IRC according to RECIST v1.1.1
CI=confidence interval; CR=complete response; IRC=independent review committee; NE=not estimable; ORR=objective response rate; PR=partial response; RECIST=Response Evaluation Criteria in Solid Tumors
Retevmo had CNS activity in patients with locally advanced or metastatic RET fusion-positive NSCLC and measurable brain metastases (n=21)1
CNS ORR was observed in the LIBRETTO-001 trial1
Of the 21 patients with measurable disease, 3 patients received RT to the brain within 2 months prior to study entry.1
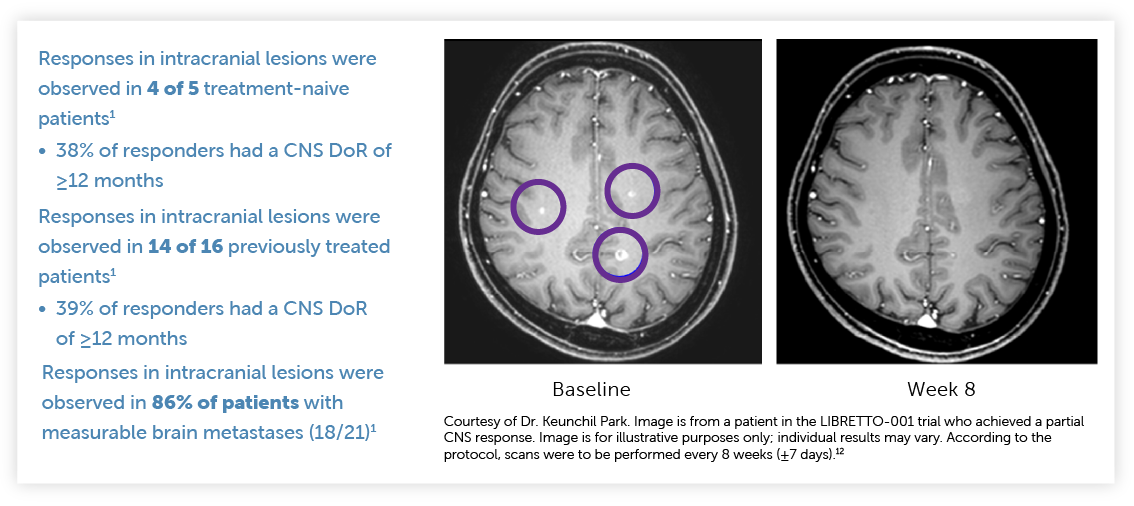
Baseline and Week 8 scans from a patient in the LIBRETTO-001 trial who achieved a partial CNS response with Retevmo.
Responses in intracranial lesions were observed in 4 of 5 treatment-naive patients. 38% of responders had a CNS DoR of ≥12 months.
Responses in intracranial lesions were observed in 14 of 16 previously treated patients. 39% of responders had a CNS DoR of ≥12 months.
Responses in intracranial lesions were observed in 86% of patients with measurable brain metastases (18/21).
CNS ORR and CNS DoR were prespecified secondary endpoints that were evaluated and confirmed by an IRC.1,13
Select Important Safety Information
Hypertension occurred in 41% of patients, including Grade 3 hypertension in 20% and Grade 4 in one (0.1%) patient. Overall, 6.3% had their dose interrupted and 1.3% had their dose reduced for hypertension. Treatment-emergent hypertension was most commonly managed with anti-hypertension medications. Do not initiate Retevmo in patients with uncontrolled hypertension. Optimize blood pressure prior to initiating Retevmo. Monitor blood pressure after 1 week, at least monthly thereafter, and as clinically indicated. Initiate or adjust anti-hypertensive therapy as appropriate. Withhold, reduce dose, or permanently discontinue Retevmo based on severity.
Retevmo was studied in 14 additional advanced or metastatic RET fusion-positive solid tumors1
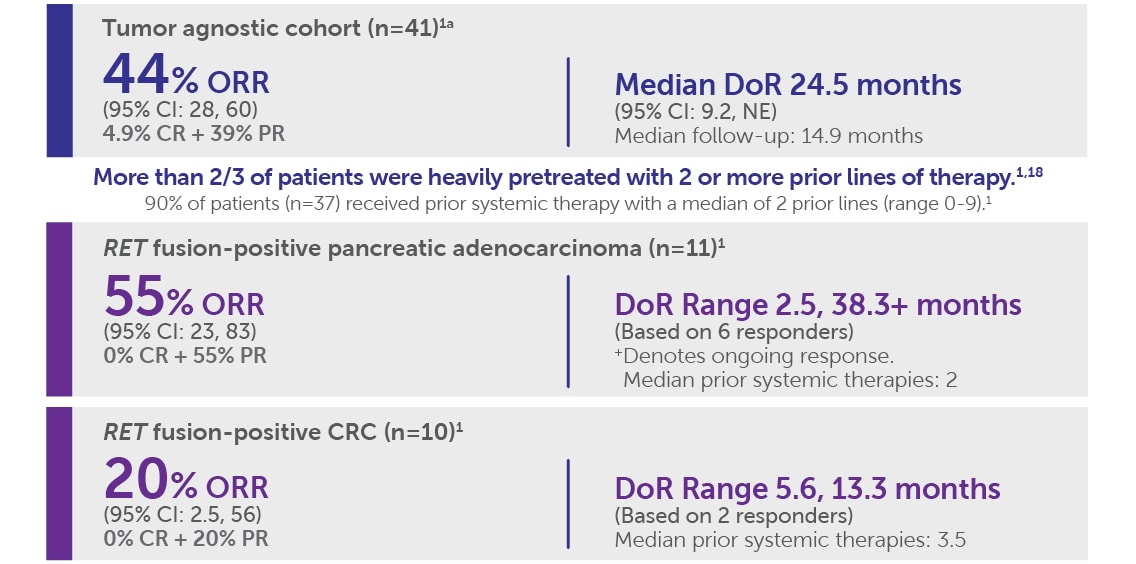
Tumor Agnostic Cohort (n=41)
- ORR was 44% (95% CI: 28, 60); 4.9% CR + 39% PR
- Median DoR was 24.5 months (95% CI: 9.2, NE)
- The median follow-up was 14.9 months
RET fusion positive pancreatic adenocarcinoma (n=11):
- ORR was 55% (95% CI: 23, 83); 0% CR + 55% PR
- DoR range was 2.5 months, 38.3+ months, based on 6 responders
- Median prior systemic therapies: 2
RET fusion-positive CRC (n=10):
- ORR was 20% (95% CI: 2.5, 56); 0% CR + 20% PR
- DoR range was 5.6 months, 13.3 months based on 2 responders
- Median prior systemic therapies: 3.5
aEfficacy was evaluated in 41 adult patients with locally advanced or metastatic RET fusion-positive solid tumors. Thirty-seven patients received systemic therapy (with a median of 2 prior systemic regimens).1
The major efficacy outcome measures in LIBRETTO-001 were ORR and DoR. At the time of analysis (September 24, 2021), 50% of responses (n=9/18) were ongoing.5
All results reviewed by an IRC.1,7
Due to rounding, numbers presented may not add up to the totals indicated and percentages may not reflect the absolute figures for the same reason.
Because Retevmo is approved across all lines of therapy, including first line in certain RET-driven cancers, consider waiting for genomic test results, including RET alteration results, before making therapeutic decisions1
Select Important Safety Information
Retevmo can cause concentration-dependent QT interval prolongation. An increase in QTcF interval to >500 ms was measured in 7% of patients and an increase in the QTcF interval of at least 60 ms over baseline was measured in 20% of patients. Retevmo has not been studied in patients with clinically significant active cardiovascular disease or recent myocardial infarction. Monitor patients who are at significant risk of developing QTc prolongation, including patients with known long QT syndromes, clinically significant bradyarrhythmias, and severe or uncontrolled heart failure. Assess QT interval, electrolytes, and thyroid-stimulating hormone (TSH) at baseline and periodically during treatment, adjusting frequency based upon risk factors including diarrhea. Correct hypokalemia, hypomagnesemia, and hypocalcemia prior to initiating Retevmo and during treatment. Monitor the QT interval more frequently when Retevmo is concomitantly administered with strong and moderate CYP3A inhibitors or drugs known to prolong QTc interval. Withhold and dose reduce or permanently discontinue Retevmo based on the severity.

Selpercatinib (Retevmo) is a National Comprehensive Cancer Network® (NCCN®)-preferred (NCCN Category 2A††) treatment option for first-line or subsequent‡‡ therapy in patients with RET-positive metastatic non-small cell lung cancer (NSCLC)19§§
NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) recommendations for NSCLC19:
Specific targeted therapies are the preferred systemic treatment options for eligible patients with metastatic NSCLC with certain driver alterations.‖‖
For patients with metastatic NSCLC who are RET rearrangement positive, NCCN NSCLC Panel recommends selpercatinib (Retevmo) as a first-line or subsequent‡‡ therapy option (category 2A††) (preferred) for patients with metastatic NSCLC who are positive for RET rearrangements.
NCCN Guidelines® recommendations for RET alteration-positive differentiated thyroid cancers20:
Selpercatinib is a recommended systemic therapy option (category 2A††) in RET fusion-positive:
- Structurally persistent/recurrent locoregional or distant metastatic (including bone or CNS metastases) papillary carcinoma, follicular carcinoma, or oncocytic carcinoma, that is not amenable to RAI therapy
Selpercatinib is a preferred systemic therapy option (category 2A††) in RET fusion-positive:
- Metastatic anaplastic carcinoma¶¶
Selpercatinib is a preferred systemic therapy option (category 1††) in RET mutation-positive medullary carcinoma##:
- Locoregional, unresectable carcinoma that is symptomatic or progressing by RECIST criteria
- Distant metastatic, asymptomatic carcinoma that is unresectable and progressing by RECIST criteria
- Distant metastatic, symptomatic or progressive carcinoma
††Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate.
‡‡If RET inhibitors have not been previously used.
§§See the NCCN Guidelines for NSCLC for detailed recommendations, including other preferred treatment options.
‖‖The NCCN Guidelines for NSCLC provide recommendations for individual biomarkers that should be tested and recommend testing techniques but do not endorse any specific commercially available biomarker assays or commercial laboratories.
¶¶Molecular testing should include BRAF, NTRK, ALK, RET, MSI, dMMR, and tumor mutational burden.
##RET somatic genotyping in patients who are germline wild-type or germline unknown.
See safety results for Retevmo
ALK=anaplastic lymphoma kinase; BRAF=v-raf murine sarcoma viral oncogene homolog B; CI=confidence interval; dMMR=DNA mismatch repair; MSI=microsatellite instability; NE=not estimable; NTRK=neurotrophic receptor tyrosine kinase.
References: 1. Retevmo (selpercatinib). Prescribing Information. Lilly USA, LLC. 2. Phase 1/2 study of LOXO-292 in patients with advanced solid tumors, RET fusion-positive solid tumors, and medullary thyroid cancer (LIBRETTO-001). https://clinicaltrials.gov/ct2/show/NCT03157128. Updated June 9, 2022. Accessed June 14, 2022. 3. Drilon A, Subbiah V, Gautschi O, et al. Durability of efficacy and safety with selpercatinib in patients with RET fusion+ non-small-cell lung cancer: LIBRETTO-001. Poster presented at: European Lung Cancer Congress; March 30–April 2, 2022. Poster 27P. 4. Data on File, Lilly USA, LLC, DOF-SE-US-0063. 5. Subbiah V, Wolf J, Konda B, et al. Tumor agnostic efficacy of selpercatinib in patients with RET fusion-positive solid tumors: a global, multicenter trial updated (LIBRETTO-001). Presented at: 2022 ASCO Annual Meeting; June 3-7, 2022; Chicago. Abstract 3094. 6. Drilon A, Oxnard GR, Tan DSW, et al. Efficacy of selpercatinib in RET fusion–positive non–small-cell lung cancer. N Engl J Med. 2020;383(9):813-824. 7. Wirth LJ, Sherman E, Robinson B, et al. Efficacy of selpercatinib in RET-altered thyroid cancers. N Engl J Med. 2020;383(9):825-835. 8. McCoy CE. Understanding the intention-to-treat principle in randomized controlled trials. West J Emerg Med. 2017;18(6):1075-1078. 9. Gupta SK. Intention-to-treat concept: a review. Perspect Clin Res. 2011;2(3):109-112. 10. Data on File, Lilly USA, LLC, DOF-SE-US-0058. 11. Data on File, Lilly USA, LLC, DOF-SE-US-0028. 12. Data on File, Lilly USA, LLC, DOF-SE-US-0013. 13. Data on File, Lilly USA, LLC, DOF-SE-US-0033. 14. Data on File, Lilly USA, LLC, DOF-SE-US-0031. 15. Data on File, Lilly USA, LLC, DOF-SE-US-0032. 16. Data on File, Lilly USA, LLC, DOF-SE-US-0024. 17. Data on File, Lilly USA, LLC, DOF-SE-US-0069. 18. Data on File, Lilly USA, LLC, DOF-SE-US-0067. 19. Referenced with permission from The NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Non-Small Cell Lung Cancer V11.2024. © National Comprehensive Cancer Network, Inc. 2024. All rights reserved. Accessed October 15, 2024. To view the most recent and complete version of the guidelines, go online to https://www.nccn.org. 20. Referenced with permission from The NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Thyroid Carcinoma V4.2024. © National Comprehensive Cancer Network, Inc. 2024. All rights reserved. Accessed Sept 23, 2024. To view the most recent and complete version of the guidelines, go online to https://www.nccn.org.
INDICATIONS
Retevmo is a kinase inhibitor indicated for the treatment of:
- adult patients with locally advanced or metastatic non-small cell lung cancer (NSCLC) with a rearranged during transfection (RET) gene fusion, as detected by an FDA-approved test
- adult and pediatric patients 2 years of age and older with advanced or metastatic medullary thyroid cancer (MTC) with a RET mutation, as detected by an FDA-approved test, who require systemic therapy
- adult and pediatric patients 2 years of age and older with advanced or metastatic thyroid cancer with a RET gene fusion, as detected by an FDA-approved test, who require systemic therapy and who are radioactive iodine-refractory (if radioactive iodine is appropriate)
- adult and pediatric patients 2 years of age and older with locally advanced or metastatic solid tumors with a RET gene fusion, as detected by an FDA-approved test, that have progressed on or following prior systemic treatment or who have no satisfactory alternative treatment options*
*This indication is approved under accelerated approval based on overall response rate (ORR) and duration of response (DoR). Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.